

Name has been changed to protect patient privacy. Clinical details and images are shared with the patient’s consent.
Ten years is a long time to wait for something you want this much.
When Kavitha reached out to us, she was 37 and had been trying to conceive for a decade. Not long before, she had finally seen a positive pregnancy test after an IUI. Then, at six weeks, the pregnancy stopped growing and she went through a miscarriage. By the time she came to Fertilia, she was carrying both the hope of starting again and the quiet ache of a loss that was still fresh.
Her fertility specialist had a clear plan: IVF would be the next step. Kavitha came to us with one simple goal before that cycle began. She wanted to walk into it with her body as ready as it could be.
For more on this, read our guide on IVF Twins at 40. This is how she got there, and how her first IVF cycle worked.
Where She Started
Kavitha is a homemaker. Her husband, 41, works in marketing. They had been married ten years and had been through the full length of a fertility journey: follicular studies done three times, a normal HSG, and an IUI that finally led to a conception, which then ended in an early miscarriage.
Kavitha’s profile at intake:
- Age: 37
- Height: 144 cm
- Weight: 63 kg (BMI: 30.4)
- Cycles: Regular, 30 days, normal flow
- Recent history: IUI conception, then a missed miscarriage at six weeks
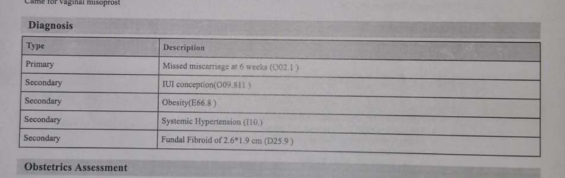
- Other findings: Systemic hypertension, a small fundal fibroid (2.6 x 1.9 cm), and a family history of hypertension (her mother)
Her diagnosis summary from the recent pregnancy loss told the fuller story: a missed miscarriage at six weeks following an IUI conception, alongside obesity, systemic hypertension, and the small fibroid.
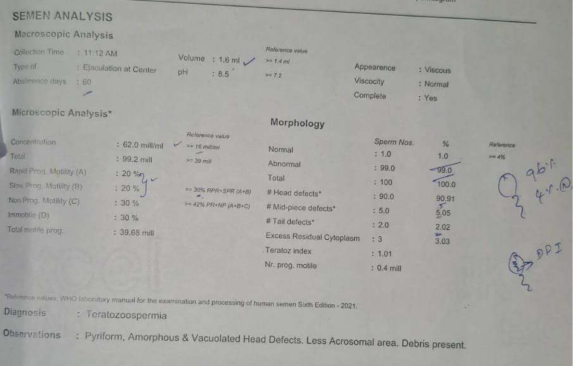
There was a second part to the picture, and it mattered. Her husband’s semen analysis showed teratozoospermia: his sperm concentration was adequate, but only about 1% of the sperm had a normal shape, against a reference of 4% or more, with a high proportion of head defects.
This is why her fertility specialist had recommended IVF. With a male-factor issue of this kind alongside ten years of trying and a recent loss, IVF gave them the most reliable path forward. None of this was a failing on anyone’s part. It was simply the clinical reality of their situation, and they were meeting it sensibly.
At 144 cm, Kavitha’s height changes how a number like 63 kg reads. The same weight sits very differently on a shorter frame, and at her height it placed her BMI at 30.4. Bringing that down was not about appearance. It was about giving the IVF cycle, and any pregnancy that followed, the steadiest possible starting conditions.
Preparing for IVF or an Embryo Transfer?
If you want to give your body the best possible chance before a cycle begins, we can help you understand which lifestyle changes genuinely matter, and which do not.
Why Preparation Came First
Many women are told, somewhere along the way, to “lose some weight before treatment.” It is sound advice, but it is rarely paired with a plan that fits a real life. Kavitha had heard versions of it before. What she had not had was someone to sit with her, look at her actual routine, and build something she could keep.
Here is what the research says about why this step is worth taking:
Weight and IVF outcomes. A higher BMI is associated with lower live birth rates in IVF cycles. This is not about how a woman looks. It reflects the metabolic and hormonal environment the embryo enters (Rittenberg et al., 2011, Human Reproduction Update). Even a modest, sustainable reduction can shift that environment in a helpful direction.
Lifestyle before the cycle. A 2020 systematic review in Human Reproduction Update found that lifestyle interventions before IVF were linked with improved clinical pregnancy rates (Lim et al., 2020). The weeks before a cycle are not waiting time. They are working time.
The whole couple, not one half. Sperm quality responds to lifestyle too. Larger reviews of dietary patterns link diets rich in vegetables, whole grains, pulses and good fats with better semen parameters (Salas-Huetos et al., 2017, Human Reproduction Update). Preparation is something a couple does together, even when only one of them is undergoing the procedure.
Kavitha’s situation touched several of these at once. So the plan was built to be steady and entirely doable, not dramatic.
The Plan: Her Own Kitchen, Rebalanced
We did not hand Kavitha an unfamiliar diet. She eats South Indian food, mostly non-vegetarian, on a settled daily rhythm: idli or dosa in the morning, rice at lunch, and a light dinner. Our nutritionist kept all of that and simply rebalanced it.
The plan was an anti-inflammatory pattern set at around 1,200 kcal, with roughly 60 g of protein, built around the foods she already cooked. The structure was simple:
- Protein at every meal to keep her full and steady: egg, dal, chana, paneer, fish or chicken
- Complex carbohydrates in measured portions: idli, dosa, and rice kept, not banned, just portioned
- Vegetables and a raw side at most meals: cucumber, salads, poriyals
- Consistent meal timings, which on their own help steady blood sugar
A few of her actual plates show how ordinary the food was.
A breakfast of dosa with a boiled egg, sambar, and sliced cucumber:

Idli with a boiled egg, a dal, and cucumber, a plate any Tamil household would recognise:

And a non-vegetarian lunch of chicken curry with a measured portion of rice and cucumber:

There was no imported superfood on any plate. No supplement shopping list. Just her own cooking, portioned and balanced, with protein brought forward and the raw vegetables built in.
Movement stayed equally familiar. Kavitha already walked in the early morning, between 6 and 6:30. We kept that habit exactly as it was and let it count, rather than asking her to add an unrealistic new routine on top of running her home.
What Changed, in About Two Months
Kavitha lost weight the way that lasts: gradually, and without going hungry.
Her weight came down from 63 kg to 57.2 kg, close to 6 kg, in roughly two months.
That loss took her BMI from 30.4 to about 27.6. More importantly, it happened with no supplements and no extreme dieting, which meant her body went into the IVF cycle nourished rather than depleted. The weight loss also gently supported her blood pressure, which mattered given her history.
She described feeling lighter and more energetic, the kind of change that does not show on a report but changes how a day feels.
The First IVF Cycle
With her body in a steadier place, Kavitha returned to her fertility specialist and began her IVF cycle.
It worked the first time.
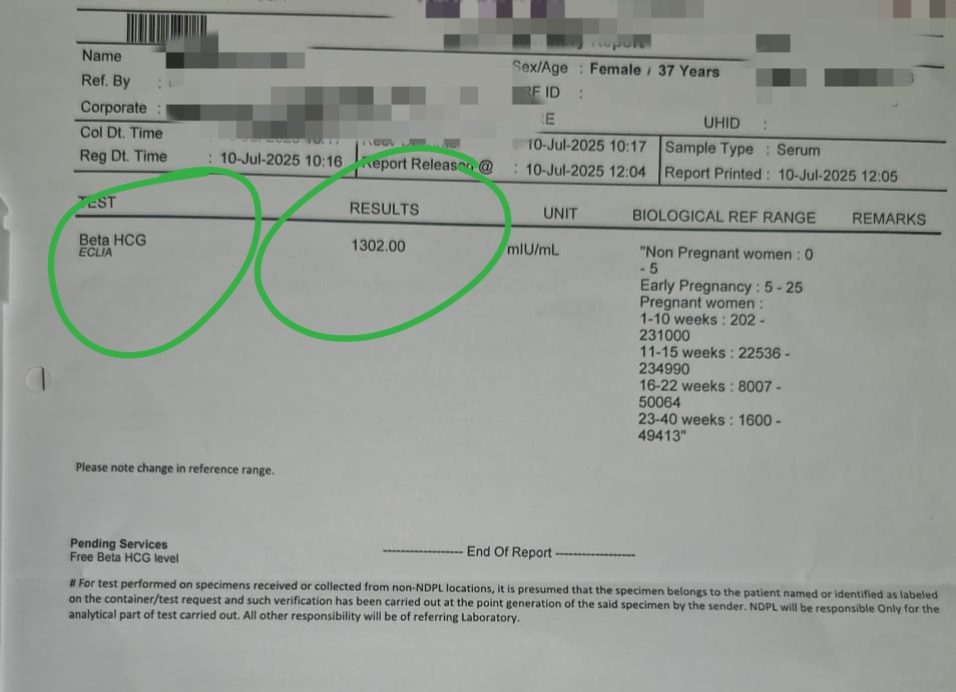
A clearly positive beta hCG of 1302 mIU/mL confirmed the pregnancy.
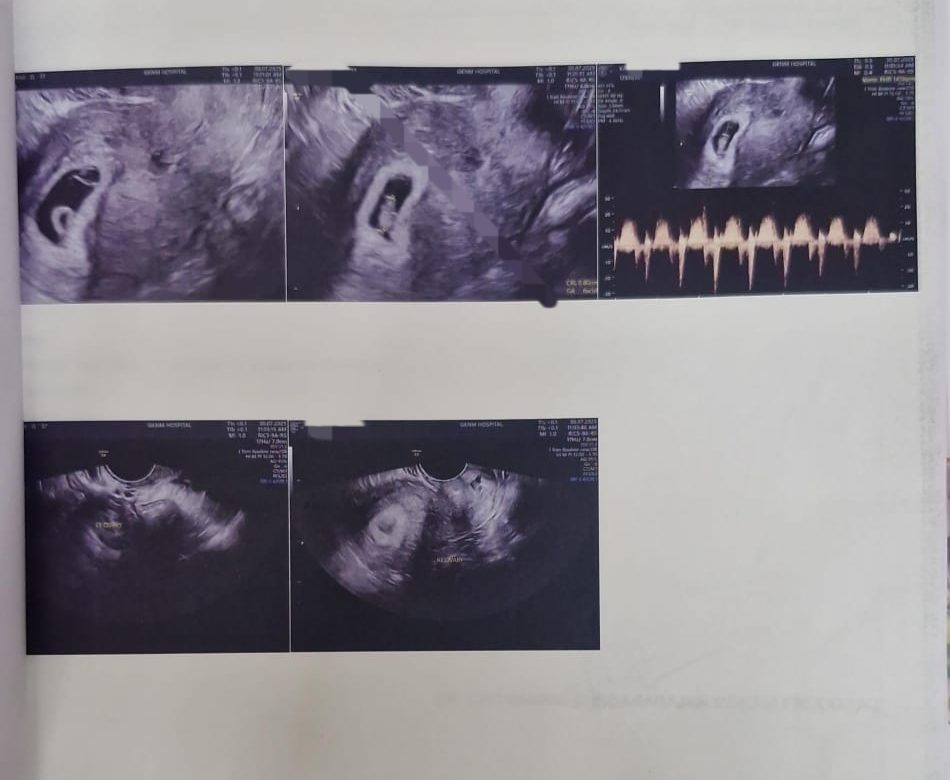
Not long after, an early scan confirmed what every couple in this position waits to see: a heartbeat.
After ten years, a loss, and a long road of tests and treatments, her first cycle succeeded. We stayed with her through those early weeks, the time when a previous loss makes every day feel longer, guiding her on food, gentle movement, and the questions that come at 2 a.m.
In Her Own Words
When we last heard from the couple, this is the message they sent. It is shared exactly as they wrote it.
“We thank the team for the guiding training programme they have provided, along with the necessary care, advice, and daily follow-ups to help us lose weight more healthily without any food supplements, dropping from 64kg to 57kg in two months. This programme also makes our body feel lighter, healthier, and more energetic.
I will recommend this programme to everyone interested in losing weight and seeking a healthier life.”
What This Story Teaches Us
1. Preparation is part of the treatment, not a delay before it
The weeks before an IVF cycle are an opportunity, not dead time. Bringing weight and metabolic health into a better place gives the cycle better conditions to work with. For Kavitha, two months of steady preparation set up a first-cycle success.
2. Height changes how a weight number reads
At 144 cm, 63 kg placed Kavitha’s BMI above 30. The same weight on a taller woman would read very differently. This is why a number on the scale means little on its own, and why a plan should be built around the person, not a generic target.
3. Fertility is a couple’s picture
Her husband’s semen analysis was a real part of why IVF was recommended. Treatment planning, and lifestyle preparation, work best when both partners are part of the conversation rather than only the woman.
4. The kitchen you already have is usually enough
Kavitha’s plates were idli, dosa, dal, egg, chicken curry, rice, and cucumber. The change was in balance and portion, not in buying anything new. A plan that lives inside the family’s normal cooking is a plan that holds.
5. A previous loss does not close the door
A miscarriage is painful, and the fear it leaves is real. Kavitha’s story is a quiet reminder that a loss can be followed by a healthy pregnancy, and that careful preparation and good care can carry a couple through to the next step.
Getting Ready for Your Own Cycle?
Every woman’s situation is different. Whether you are heading into your first IVF cycle or trying again after a loss, getting your body ready beforehand can make a meaningful difference. We work alongside your fertility specialist, never in place of them.
Frequently Asked Questions
Does losing weight before IVF improve the chances of success?
It can. Research consistently links a higher BMI with lower live birth rates in IVF, and even a modest, sustainable reduction can improve the metabolic and hormonal environment an embryo enters (Rittenberg et al., 2011, Human Reproduction Update). A 2020 review also found that lifestyle changes before a cycle were associated with better clinical pregnancy rates (Lim et al., 2020). Kavitha’s roughly 6 kg loss brought her BMI from 30.4 to about 27.6 before her cycle. Because each IVF cycle is a significant emotional and financial investment (here is what IVF actually costs in India), giving your body its best chance first is time well spent.
How can 63 kg be classified as obese?
Body mass index accounts for height, not just weight. At 144 cm, Kavitha’s 63 kg gave a BMI of 30.4, which crosses the obesity threshold, whereas the same weight on a taller woman would read as a healthy BMI. This is why weight targets should always be set against your own height and build, not against a single number.
What does teratozoospermia mean, and can IVF still work?
Teratozoospermia means a high proportion of sperm have an abnormal shape (morphology), which can affect their ability to fertilise an egg naturally. It is one reason a fertility specialist may recommend IVF, where fertilisation can be supported directly. It does not mean pregnancy is impossible. Diet and lifestyle can also support semen quality over time (Salas-Huetos et al., 2017), which is why preparation is something couples do together.
Is it safe to try again so soon after a miscarriage?
The right timing after a miscarriage depends on your individual situation, and your treating doctor will guide you on when to begin. Using the time in between to prepare your body, with balanced nutrition and gentle movement, is a constructive way to move forward while you wait for the green light to start a cycle.
Was Kavitha on any supplements or medication to lose the weight?
No. Her weight loss came entirely from rebalanced home-cooked food and her existing morning walk, with daily follow-ups from our team. As her own message says, the change happened “without any food supplements.” Any medication for her blood pressure or fertility cycle was managed by her treating doctors.
How long does it take to prepare for IVF?
It varies. Some metabolic improvements show within weeks, while egg and sperm development happen over roughly two to three months, so a longer runway can help. Kavitha saw meaningful change in about two months. Even a shorter window is worthwhile, because the goal is a steadier starting point, not perfection.
Does Fertilia replace my IVF doctor?
Not at all. Your fertility specialist runs the medical side of IVF: the stimulation, the retrieval, the transfer. We handle the lifestyle layer alongside them, nutrition, movement, and daily support, so that your body is as ready as possible. The two work together. Kavitha’s specialist managed her cycle while we helped her prepare for it and supported her through the early weeks afterwards.
Related Case Studies
- How Madhu’s embryo transfer succeeded. After a failed transfer, Madhu lost 6 kg and brought her blood sugar into a healthy range in one month. Her second transfer succeeded.
- HbA1c 9.8 to pregnancy. Gowri was referred to us by her own doctor to prepare before fertility treatment, and conceived after three months of metabolic work.
- How Fertilia supports IVF journeys: five real stories. Five women across the three windows where IVF preparation matters most.
This is part of a series of patient case studies from our clinic. Every story is real, verified, and shared with the patient’s explicit consent. Names and identifying details are changed to protect privacy.
Dr. Suganya Venkat is an OB-GYN with 15+ years of experience. She holds an MBBS (SRMC, 5 Gold Medals), MD in Pathology (CMC Vellore), and DNB in OB-GYN (GKNM Hospital, Coimbatore).



